
Novartis
OOH
IG Posts

Why Testing?
Because some genes deserve a second look.
Every family has its phrases that turn something worth noticing into ordinary.
“High cholesterol runs in the family.”
“Your grandfather had heart trouble, too.”
“That’s just how it is for us.”
But familiar is not the same as harmless, and early is not the same as normal.
You deserve to know more.
The cholesterol number your doctor probably hasn’t told you about.
1 in 5 people carry it. Most will never know — until their heart tells them. A single blood test, once in your life, can change that.
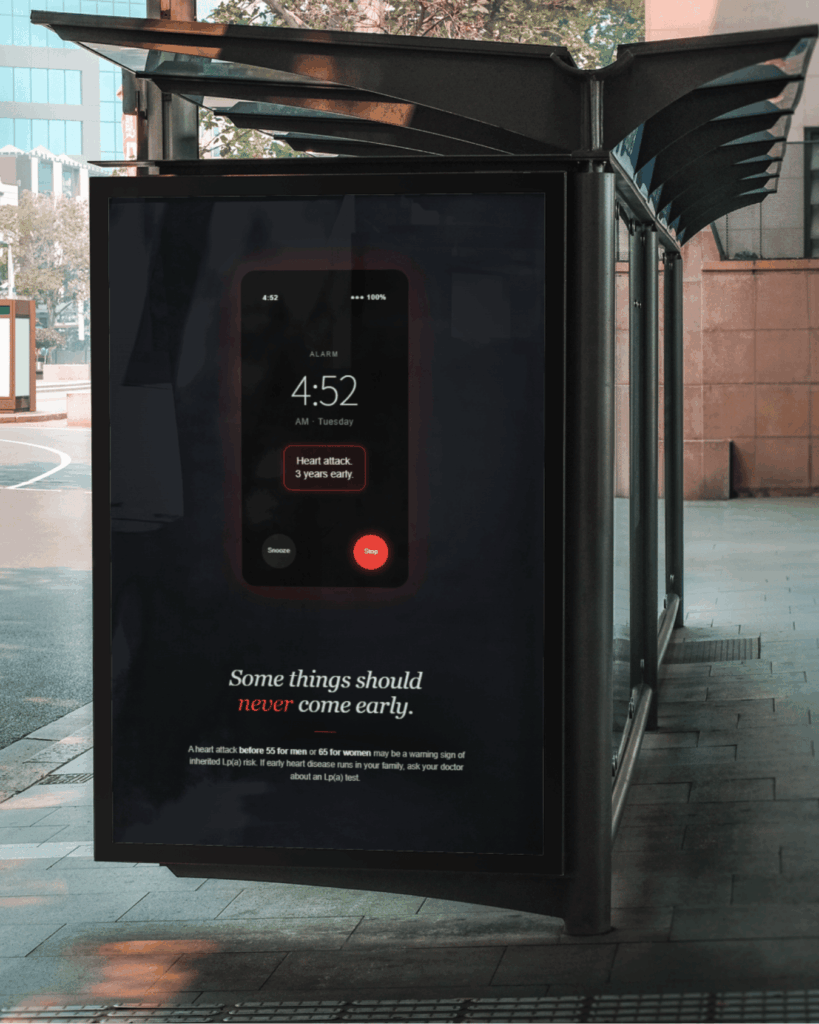
3 years early.
A particle that looks like cholesterol — but acts like a saboteur.
Lipoprotein(a), or Lp(a), is an LDL-like cholesterol particle with one crucial difference: it carries an extra protein called apolipoprotein(a) wrapped around it.
That extra protein is what makes Lp(a) uniquely dangerous. It promotes inflammation in artery walls, makes blood more likely to clot, and helps cholesterol build up where it shouldn’t. Research suggests each Lp(a) particle is roughly 6× more atherogenic than ordinary LDL.
-
A
LDL core A standard cholesterol center — same as what a regular lipid panel measures.
-
B
ApoB protein shell The structural protein that lets the particle dock with artery walls.
-
C
apo(a) — the rogue tail Found only on Lp(a). Promotes clotting, inflammation, and plaque formation. Genetically inherited.
Your cholesterol panel might be hiding something.
Standard lipid tests don’t measure Lp(a). You could have “normal” cholesterol and still carry a serious, inherited risk — the kind that shows up as an early heart attack or stroke decades before you’d expect one.
What it tells you
Total cholesterol, LDL (“bad”), HDL (“good”), and triglycerides. These respond to diet, exercise, weight, and statins. They form the basis of most routine cardiovascular risk scoring.
An entirely separate risk, sitting in plain sight.
Lp(a) is genetically fixed. Diet, exercise, and most statins don’t meaningfully change it. Someone with textbook-perfect LDL can still have dangerously high Lp(a) — and no standard screening would catch it.
Lp(a) is inherited the way eye color is — passed down, not earned.
Because Lp(a) is written into your genes in an autosomal dominant pattern, one elevated parent means roughly a 50% chance for each child. If early heart disease runs in your family, this is often why.
If one first-degree relative — a parent, sibling, or child — has elevated Lp(a) or had a heart attack early (before 55 for men, 65 for women), your own odds of carrying it are substantially higher. Clinicians call this cascade screening: one positive test in the family becomes a reason for everyone else to check.
Short answer: nearly everyone — but especially you if…
The 2026 ACC/AHA dyslipidemia guideline now recommends every adult measure Lp(a) at least once. These groups should move it up the list.
Family history of early heart disease
A parent, sibling, or child who had a heart attack, stroke, or bypass surgery before age 55 (men) or 65 (women).
A close relative with elevated Lp(a)
If anyone in your immediate family has tested high, your risk of carrying it is roughly 1 in 2. This is when cascade screening kicks in.
Personal early cardiovascular event
If you’ve had a heart attack, stroke, or significant plaque found young — Lp(a) testing can help explain why, and guide how aggressively to treat other risks.
Known high cholesterol that’s hard to control
If you’ve been on statins and your LDL still won’t cooperate, or you have familial hypercholesterolemia — Lp(a) is often the missing piece.
One vial of blood. Once in your life.
Because Lp(a) is genetic and stable, a single measurement in adulthood is usually enough to know your lifelong baseline. Most labs run it alongside a standard lipid panel.
Ask your doctor
Bring it up at your next annual visit or physical. Ask specifically for “lipoprotein(a)” — it is not included in a standard cholesterol test. Mention any family history of early heart disease.
Standard blood draw
A regular venous blood sample, no fasting required. The lab reports a number in either mg/dL or nmol/L. Above 50 mg/dL (≈125 nmol/L) is generally considered elevated.
Use the number
If it’s elevated, there’s no targeted drug yet — but the finding intensifies treatment of every other risk factor you can change: LDL, blood pressure, smoking, weight. And it flags relatives who should test too.
Things people ask — often after they’ve been diagnosed.
Some things should never come early.
A heart attack before 55 for men or 65 for women can be a sign of inherited Lp(a) risk. The test takes minutes. The knowledge lasts a lifetime.